
The Myomonitor model J1 (1967)
More than 50 years ago, Bernard Jankelson introduced a new device to relax chewing muscles, the Myomonitor. At the peak of the gnathologic era, colleagues in search of the terminal hinge axis could not understand the use of such a device for the most part and this marked the beginning of a different understanding of how the mandibular movement system functions. Gnathologists viewing the TMJ’s as mechanical guides, postulated that the mandible follows a circular path upon closure with the hinge axis at its center. Neuromuscular dentists on the other hand were (and are) convinced that the intercuspation of the teeth can be exactly hit by a mandibular movement guided by afferent and efferent neuromuscular reflexes, regardless where it is located with regard to any hinge axes.
This opened the door to the concept of „accommodation", a process by which mandibular closure accurately meets the intercuspal position even if the physiological path of the natural muscle vectors does not lead there. Actually, more often than not the path of closure does follow physiologic vectors, but the starting point of the closure (with the mandible at rest) is shifted in order to accomplish this. Nice as this sounds, it necessitates holding the mandible at rest somewhere else than where it would relax and brings with it chronic muscle tension which remains active, even when the patient does not bite on his teeth, i. e. all the time!
Jankelson had realized this and tried to find a way to restore true, so called „physiologic“ rest by relaxing the muscles positioning the mandible at accommodated rest. That low-frequency TENS with single impulses of relatively long duration (500 µsec) are effective means to this end is a well-established fact today, with more than 30 published studies citing over 200 secondary references having been collected by the manufacturer of the Myomonitor, Myo-Trinics, Inc.
Yet, it has never been quite clear what exactly the mechanisms are. Blood flow is increased so that more oxygen reaches muscle cells and more waste products, mostly of an acidic nature, are removed. Next to such histochemical changes in the tissues the release of endorphins may play a role. However, in reference to TENS, one usually finds a 1965 publication by Melzack and Wall quoted, „Pain Mechanisms: A new Theory“. Here the authors describe their „Gate Control Theory“: Non painful stimuli, conducted via fast, myelinated nerve fibers, reach the synapse before pain signals arrive along slow unmyelinated fibers and block it. They „close the gate“ to pain.
Yet we are not talking about pain here and a stimulation frequency of typically <1 Hz is unlikely to hold any gates closed. In a German publication in the ICCMO-Kompendium I therefore proposed a different theory: The slow individual impulses (in the case of the Myomonitor 0,75 Hz) actually cause movement in the stimulated muscles. These movements are of a ballistic nature, meaning that they are characterized by an initial sudden acceleration and a continuation of movement even after force is no longer applied. This is the exact opposite to isometric contractions known for their stimulation of muscle cell hypertrophy due to muscle exhaustion. In turn, the opposite of exhaustion is relaxation which is here accomplished by providing the minimal movement necessary to improve mircocirculation in the muscle while stressing muscle cells as little as possible. The quintessence of this theory is
Relaxation through Movement.
What if movement is provided in some other way?
We decided to investigate this question during a myocentric seminar as I teach at the Institut für Temporo-Mandibuläre Regulation (www.cmd.academy) since 1986. One participant suffered from chronic pain since she had subjected to an orthodontic treatment many years earlier. During her training as a dentist and during later post-graduate seminars, she had been unable to find satisfactory relief from her CMD symptoms. She volunteered as a subject for a pilot experiment which was witnessed by all course participants.
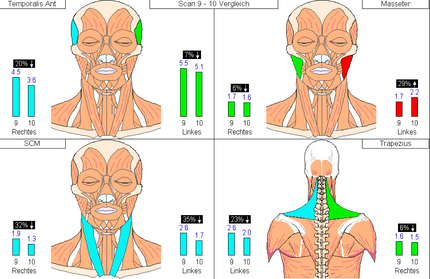
First, the base resting activity of four chewing muscles and four muscles of the neck was established with her sitting upright in a chair. The activity was monitored for several minutes, with her eyes open and closed and slight modifications to her sitting position, until the lowest attainable values were recorded for 15 seconds.
The muscles monitored were temporalis anterior (TA) left and right, masseter (MM) left and right, sterno-cleido-mastoideus (SM) left and right and trapezius (TR) left and right. The numbers under the labels on the left denote the normal values for each muscle.
Next, she placed a FreeBite air CMD between her teeth. She tried it upside-down and chose the more comfortable position (the upper and lower sides of the FreeBite are not mirror images of each other). She moved the FreeBite such that it supported her back teeth evenly on both sides and that she did not bite onto the anterior connecting tube with her incisors. She then lightly chewed on the FreeBite, opening her mouth every 3-4 chewing strokes to reposition the FreeBite with her tongue for optimal support of her back teeth. After 15 minutes, the FreeBite was removed from the mouth and the EMG-measurement was repeated employing the same protocol as before:
Within 15 minutes of lightly chewing on the FreeBite air CMD, which has a slight wedge shape insuring first contact on the back teeth, but a soft and compressible air-filling, the resting activity had dropped as much as 63%. Interestingly, even the resting tone of the monitored neck muscles responded even though no therapy had been applied there.
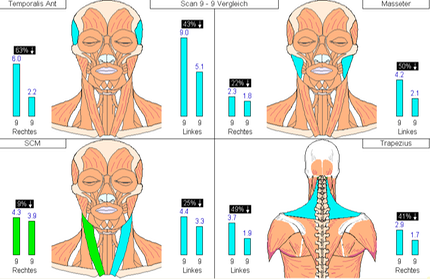
As would be expected, the change in pull on the mandible by muscles at rest resulted in a different mandibular posture. When she closed lightly on her teeth she was surprised to find out that she had contact only on one side and considerable effort was needed to bring the other side together.
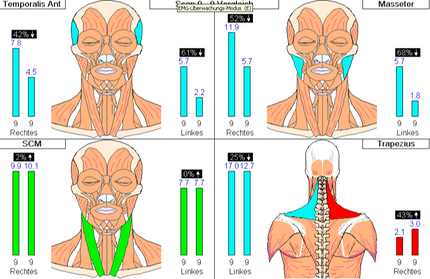
On the next day of the seminar we wanted to investigate the effects of TENS by comparison. Since new electrodes had to be applied a new resting EMG had to be taken in order to establish a reference for further measurements. However, the same protocol as on the previous day now led to different results:
Where on the previous day the average for LTA before treatment had been 9 µV, it now was 5.5 µV. In most of the other seven muscles a lower resting activity was prevalent as well. It turned out that she had worn the FreeBite through the night, because she felt the posterior support it provided comforting. This may be the reason why a lower pre-treatment resting activity resulted.
However, TENS was now applied for 50 minutes to her chewing musculature at 0.75 Hz using a pulse width of 500 µSek. In order to prevent tooth contact during treatment, the FreeBite air CMD remained between her teeth during this time.
An additional relaxation was accomplished by the TENS-therapy which is more easily seen in this comparison chart with the pre-treatment 15-second-samples depicted as the column on the left and the post-treatment values on the right next to each muscle measured:
In the meantime, we have recorded such measurements with quite a few patients. The most noteworthy may be a lady coming to my office from Switzerland. She was not too excited in trying muscle relaxation using the FreeBite, because she sells TENS-units in Switzerland for muscle relaxation for a living. She has an interesting history, since sought help with clicking in the TMJ’s by a much published dentist 15 years earlier and was told that no treatment was required since evidence-based studies have shown clicking joints to be quite normal. However, she began to develop closed locks some months later which proved increasingly difficult to treat until she finally had to subject herself to several surgical interventions in her TMJ’s. 10 years earlier I had, with some effort, managed to get her comfortable on a bite splint. She had been wearing that ever since, but it was now so worn that the occlusal surfaces were perforated in several places so that a renewal was inevitable.
The patient was unwilling to continue chewing on the FreeBite air CMD after 10 minutes and yet a significant effect had been accomplished by this time:
At this point, only her canines touched her splint anymore after she removed the FreeBite from her mouth, and she was unable to find contact on her back teeth. 40 minutes of TENS-therapy of her chewing muscles (2 channels) resulted in a further reduction of the resting activities in her chewing muscles:
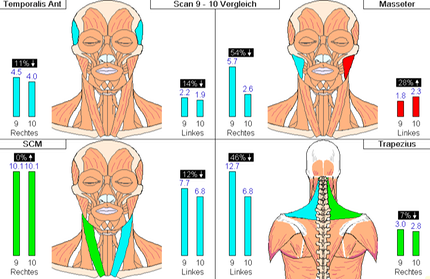
TENS, in this case, was able to restore almost perfect symmetry in the masseter muscles. However, to achieve this, the therapy took four times as long as simple chewing on the FreeBite. Multiple trials have shown with other patients that extending the duration of FreeBite-chewing beyond 30 minutes will not yield a better result in most cases. 10-15 minutes seems sufficient to accomplish a significant reduction in resting activity of the chewing muscles. The shifts produced in mandibular posture are similar to those produced by TENS in the cases studied.
In summary, we did not compare how FreeBite-chewing compares to TENS using the same time frame of therapy. However, one would not expect 10 minutes of low-frequency TENS to accomplish much in the way of muscle relaxation, while 10 minutes of FreeBite-chewing clearly does. However, TENS-therapy, if given enough time, may provide additional benifits and is therefore still part of the standard treatment protocol in my office for muscle relaxation. With patients who do not tolerate TENS well, or where TENS is contraindicated, f. i. due to a pacemaker, or when 40-60 minutes of therapy time are not avaliable, we are happy to have found a viable alternative way of relaxing chewing muscles.
