
If you run into statements such as that teeth, tooth position and the bite have little or nothing to do with TMJ dysfunction, they usually represent a certain helplessness. Gnathologic techniques are in use since the 1940s where the dentist pushes the patient’s mandible out of the naturally developed alignment in the bite, in search of an axis of vertical movement called „hinge axis“. One might actually wonder if this dysfunction has not increased in proportion to how readily the bite of a patient is changed, be it for orthodontic or prostodontic reasons. But, rather than questioning common practice, blame is being assigned to emotional, hormonal or even genetic factors as being the cause of the growing numbers of patients suffering from TMJ dysfunction.
The term itself is not well-chosen, because rarely are the TMJ’s at the center of the problem. Most of the time it is the muscles which no longer can relax, causing a chronic overload in the joints. But there is little sense in finding a statistical culprit, anyway, because the dentist or therapist is not treating numbers, but individuals and each one of them might well be the exception to the rule.
The occlusion of the teeth is part of a complicated articulation system which defines the alignment of the mandible in the bite around three axes of orientation (pitch, yaw and roll) in a defined position in space in three dimensions. One function of the bite which is commonly overlooked, as it is during discussions about most body systems, is adaptability. Our bodies are not only designed to work well, but to continue doing so, even under very adverse conditions. If the TMJ’s would guide the movement of the mandible, as gnathologic doctrine states, the teeth could no longer interdigitate in the bite once they have shifted their position as happens when a tooth is lost and neighboring teeth move into the gap. A different position of maximal intercuspation would result which could no longer be reached if the TMJ's were actually dictating movement as the joints in a dental articulator are. The human chewing system functions much more subtly than that, including not only teeth which can adjust their position in the mandibular bone, but joints which can alter their shape and movements according to functional requirements. And, last not least, a neuromuscular movement system employing reflective feedback, more resembling servo-controlled motors than mere force generators, stupidly pulling into the direction dictated by the joints as was implied by the great B. McColum, the father of Gnathology.
B. Jankelson recognized adaptability as a part of mandibular function early on and called it „mandibular accommodation“. The great difference of his myocentric protocol is that it calls for the release of such compensations before assessing a bite. What is done more thoroughly by employing TENS in order to directly treat the involved muscles can also be approximated by removing the point of intercuspation as a target for mandibular movement temporarily and observing how the muscles position the mandible in absence of a defined endpoint to mandibular movement. The FreeBite was developed with the particular accommodation of joint compression in mind, which is frequently found found in TMJ-patients. Its left and right bite cushion communicate to equalize pressure, as with the Aqualizer® and the AquaSplint®, but they extend further back towards the force vectors of the chewing muscles and the bite cushions are actually thickest between the back teeth, reminding the neuromuscular system with every bite that no joint compression is required to find posterior support.
While there can be little debate as to the effectiveness of such bite cushions in the treatment of TMJ dysfunction, a recent discussion with a patient demonstrated to me, that the exact mechanical properties of these devices are all but unknown. He wanted a bite cushion which would increase the vertical dimension of the bite by no more than 2 mm at the most and had found such dimensions given somewhere on the internet.
But obviously such an increase of vertical dimension is dependent on several factors. A water-filled device will mold itself to the occlusal surfaces of the teeth as bite force increases, but then compress no more, as long as its casing will not stretch. By contrast the air-filling of the FreeBite air remains compressible, even after the device has molded itself to the teeth. In addition, the Aqualizer® is known to progressively lose water and with it effective height, so that the age of the device has a significant influence on its effective height, also necessitating its frequent replacement.

Test setup employing the Myotronics K7 system
We therefore decided to study the effective height of the three mentioned devices under well controlled clinical conditions directly in the patient’s mouth while monitoring bite strength electromyographically. A patient was connected to a K7 system (Myotronics, Inc.) which allows for simultaneous measurement of mandibular position and electrical muscle activity (EMG signal). The latter does not directly represent bite force, but gives a proportional value, meaning that twice the EMG amplitude roughly represents twice the bite force. Since the ratio between EMG-amplitude and bite force in an individual is usually not known, force is customarily expressed in % MVC (maximal voluntary contraction). In this experiment MVC was assessed by the subject biting three times onto cotton rolls with maximal strength and using the rectified mean square of the highest of the three attempts as measured in the M. masseter on the stronger side (in this case 300 µV). The experiment with the bite cushions were conducted with a force representing ⅙ MVC (50 µV) which was deemed sufficient to mold the bite cushions to the teeth, but not enough to rupture or cause deformation of the casing in any of them.

Use of the monitor as a bio-feedback device to insure a controlled bite force.
The mandibular position was recorded at light contact with the bite cushion, at ⅙ MVC and in maximal intercuspation directly on the teeth. Several series were recorded using the same subject and the results then averaged. During the bite with ⅙ MVC onto each device the subject observed his EMG signal on the screen, adjusting his muscle tension until an amplitude of 50 µV was reached and the mandibular position was recorded at that time.

Aqualizer, AquaSplint and FreeBite line-up
The tests included the regular size of the Aqualizer® termed „ultra“, one each in the volumes „low“, „medium“ and „high“. Furthermore, an AquaSplint® mini was tested and finally the FreeBite® air CCD, CCD low and CMD as well as the water-filled FreeBite® balance CCD, CCD low, CMD and CMD low. All devices were new.
Depending on the shape of the dental arch, the bite cushions reach the area of the first molars with the Aqualizer® ultra while those of the Aqualizer® mini (not tested) and AquaSplint® mini end in the premolar region. The bite cushions of the FreeBite® extend to the distal ends of the dental arches. It can be expected that due to these differences alone the devices have different mechanical properties in the mouth, dependent on the shape of the dental arch of the wearer. The test series therefore was carried out with the same subject in order to eliminate those variables.
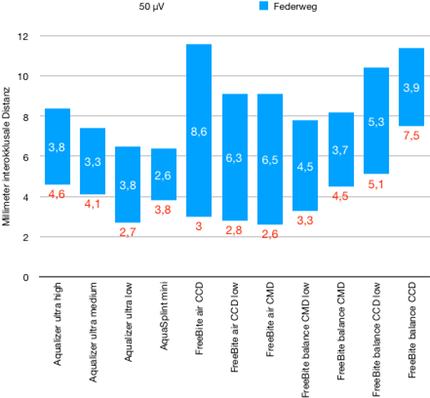
In the diagram each blue column represents the travel from light contact between the teeth and the bite cushion of each device to 50 µV or ⅙ MVC. The effective vertical gain at ⅙ MVC of each device is represented by the red numbers in mm interocclusal distance. The line y=0 represents maximal intercuspation of the teeth (interocclusal distance = 0 mm).
As can readily be seen, there is no Aqualizer® raising the bite less than 2 mm, as the patient had seen on the internet. The deviations between the trials are not depicted in this graph. As expected, they are less the more repetitive the device can be placed in the mouth. The least variation was observed with the AquaSplint® mini after the device was shaped to the lower dental arch by bending its stainless steel wire accordingly. The FreeBite® follows an entirely different concept where emphasis is not placed upon a secured position in the mouth, or even on maximizing comfort of wear over extended time periods. Rather, the design favors a maximal therapeutic effect in the shortest possible time, especially with regard to compression of the TMJ’s. The device is designed to encourage playful movement by lightly chewing on it (like a bi-lateral chewing gum) while slightly moving it from one position to another with the tongue. In a clinical setting such a „therapy“ may last 5-15 minutes while the patient can extend the sessions at home. The attempt to wear a FreeBite for many hours, such as through the night, is recommended only after the patient has learned not to clench on it when no longer playfully moving.
By far the largest travel was recorded with the FreeBite® air CCD (8.6 mm). Air-filled devices can be expected to compress in proportion to the force exerted upon them. Conversely, much less additional compression was observed with water-filled devices, as also is expressed in the travel of only 3.9 mm measured with the FreeBite® balance CCD, even though the vertical dimension at light contact was very similar. Future studies will be dedicated to those mechanical properties including the behavior of the devices under heavy load near MVC.
Averaged and rounded, the following summary can be given in regard to the effective height of different bite cushions as tested in the mouth at a closely controlled compressive force:
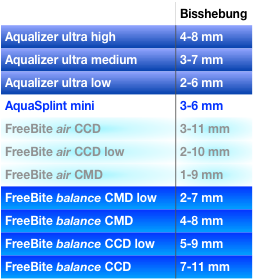
„Bisshöhe" = effective vertical gain in mm of new Aqualizers, AquaSplint mini and FreeBites in a direct comparison.